
Annual report 2017: England, Northern Ireland, Scotland and Wales
Date of publication: October 2017
Our 2017 annual report provides findings relating to people who died by suicide or were convicted of homicide in 2005-2015 across all UK countries. Additional findings are presented on sudden unexplained deaths (SUD) under mental health care in England and Wales.
Our large, internationally unique database is a national case series of suicide, homicide and SUD by mental health patients. This allows us to examine the circumstances surrounding these incidents and changes in trends over time, and to make recommendations for clinical practice and policy to improve safety in mental health care.
Key messages
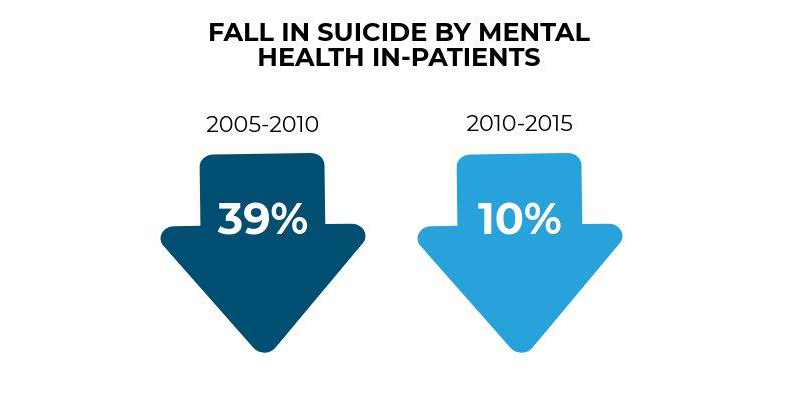
In-patient care
Suicide by people under in-patient care has been falling over the last 10 years, but the rate of decline is slowing.
There should be a renewed emphasis on suicide prevention on in-patient wards, with the aim of re-establishing the previous rate of decrease in in-patient suicide.
This could include:
- measures to improve the physical environment, eg removing low-lying ligature points;
- ensuring care plans are in place during agreed leave;
- measures to reduce leaving the ward without agreement, eg improvements to ward milieu, better monitoring of ward access and exit points, and observation protocols.
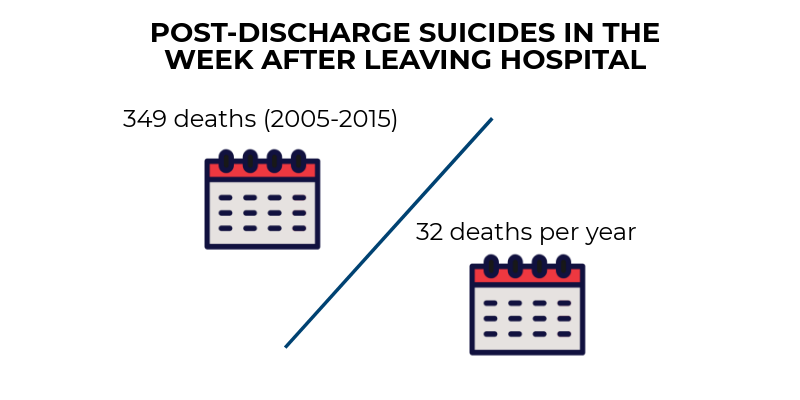
Post-discharge care
The days following discharge from in-patient care are a time of particularly high risk. We recommend patients leaving in-patient care be followed up by the service as soon as possible – ideally within three days of discharge. A care plan should also be in place at the time of discharge from hospital.
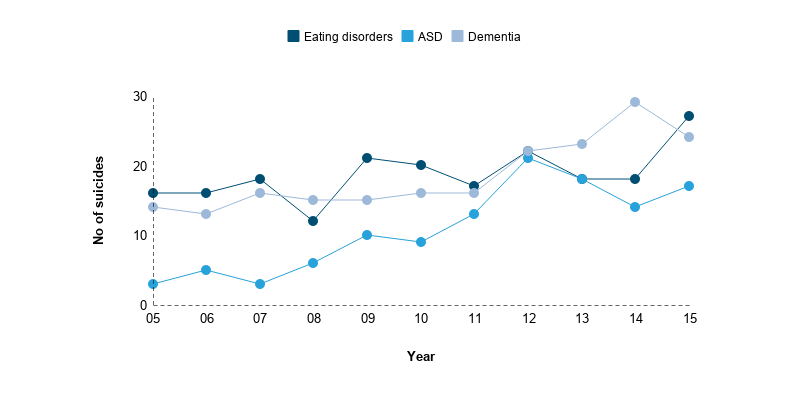
Diagnostic groups
The number of suicides with a diagnosis of eating disorder, autism spectrum disorder or dementia has risen. Although this is likely to reflect a rising number of patients with these diagnoses under mental health care, we ask clinicians to be aware that patients with these diagnoses may feel suicidal.
We recommend mental health staff have access to specialist support in treating patients with these diagnoses.
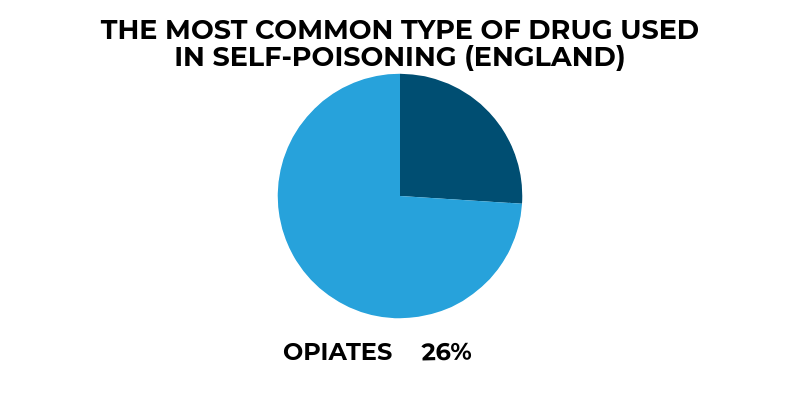
Reducing suicide by opiate overdose
The most common drugs used in self-poisoning are opiates, and the number of deaths by opiate poisoning is rising. Clinicians and pharmacists should be aware of the potential risks of opiate and opiate-containing analgesics.
Safer prescribing in primary and secondary care remains crucial, particularly for patients with long-term pain, a group who are at high suicide risk. We recommend that only short-term supplies be prescribed or kept at home.
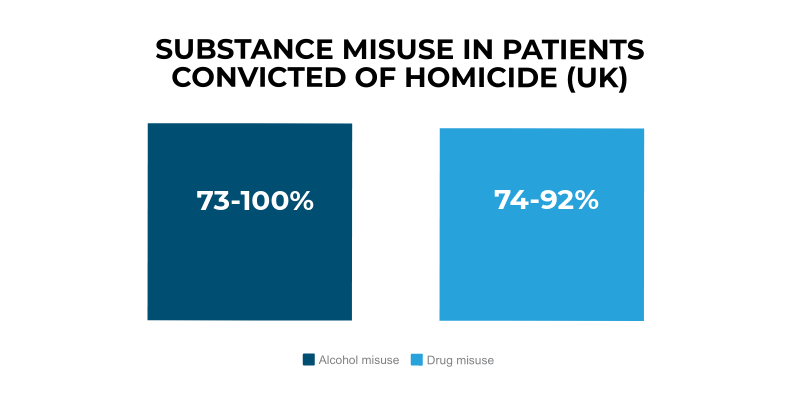
Alcohol and drug misuse
Our findings add to the evidence that much of the risk to others from mental health patients is related to co-existing drug or alcohol misuse rather than mental illness itself. This is an important message in combating stigma.
We recommend a greater focus on alcohol and drug misuse in risk management in mental health care, with specialist substance misuse and mental health services working closely together.
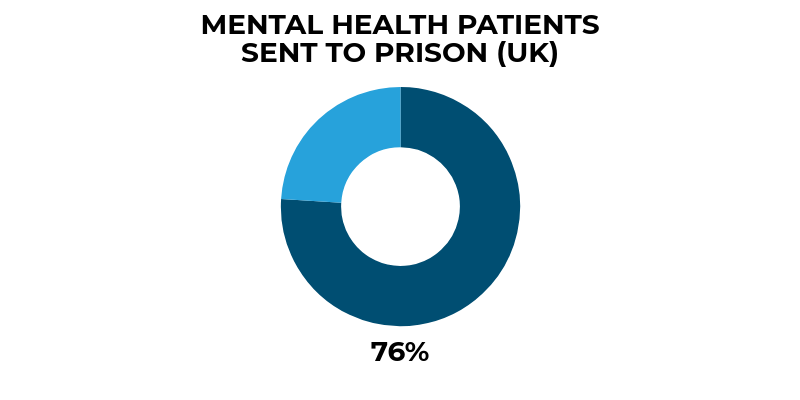
Patient homicides and courts
Our findings raise concerns about patients with severe mental illness being sent to prison rather than hospital following conviction for homicide. Further investigation of whether these decisions are appropriate should now be undertaken by health and justice agencies.
Find out more
Contact Us
+44 (0) 161 306 6000