
Annual report 2021: England, Northern Ireland, Scotland and Wales
Date of publication: May 2021
Our 2021 annual report provides findings relating to people who died by suicide between 2008 and 2018 across all UK countries. Additional findings are presented on the number of people under mental health care who have been convicted of homicide, and those in the general population.
Our large and internationally unique database is a national case series of suicide by patients under the care of mental health services over more than 20 years. This allows us to make recommendations for clinical practice and policy that will improve safety locally, nationally, and internationally.
Some of the people most affected by the COVID-19 pandemic – young people, ethnic minorities, people who live alone – have also been a concern in suicide prevention. Their mental health will be an important feature of society’s recovery. In this report, we do not yet have data from 2020, but our findings highlight key issues in patient safety in these groups.
Key messages
Patients who live alone
There were 746 deaths per year by patients who lived alone, nearly half (48%) of all patient suicides. These patients were more often aged over 45, unemployed, single or widowed, and had experienced recent financial difficulties and relationship break-up more often than those who did not live alone.
We suggest clinical services should be aware of the vulnerability of patients who live alone, and care packages devised by clinical services and other agencies for these patients should address these clinical and social risks.
Patients from ethnic minority groups
 Our findings show differences between ethnic groups in social and clinical characteristics that could be important to suicide prevention:
Our findings show differences between ethnic groups in social and clinical characteristics that could be important to suicide prevention:
- South Asian patients were less likely to be unmarried or living alone, and they had high rates of affective disorder;
- Black Caribbean and Black African patients were more likely to live alone and had the highest rates of schizophrenia and other delusional disorders and previous violence. Black Caribbean patients also had higher rates of substance misuse;
- Chinese patients were more often female and had a short history of psychiatric illness;
- patients from a multiple/mixed ethnic background had higher rates of personality disorder, co-morbidity, and previous self-harm and substance misuse.
We ask clinical services to be aware that the suicide risk profile of patients differs between ethnic groups, and we recommend different suicide prevention approaches in relation to severe mental illness or depression, alcohol or drug misuse, likely suicide method, or recent migration.
People aged under 25

Between 2008 and 2018, the number of young patients who died by suicide increased, particularly in those aged 15-17 and in female patients.
We recommend that clinical services should:
- have the breadth of skills to respond to the clinical complexity of many younger patients, including combinations of personality disorder diagnosis, eating disorders, self-harm, and substance misuse;
- ensure these co-morbidities don’t act as a reason for non-acceptance by services designed for single conditions.
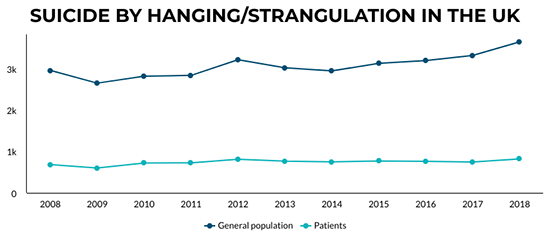
Methods of suicide
Our findings show a continuing increase in the number of deaths by hanging/strangulation among patients under mental health care. This is a difficult method to prevent outside institutional settings.
We recommend clinicians assessing risk consider the factors associated with this method; recent risk factors such as self-harm, adverse life events and diagnosis of depression; and apparent protective factors such as employment and marriage.
Suicide prevention during COVID-19
 For many people with mental ill-health, the pandemic has brought new stresses and disruption to daily life and the availability of care. In a pilot data collection of real-time surveillance of suspected suicide, we were notified of 133 deaths by mental health trusts in England between 23 March and 30 September 2020. Most deaths occurred in community settings, and over a third of clinicians reported disruption to the patient’s usual mental health care.
For many people with mental ill-health, the pandemic has brought new stresses and disruption to daily life and the availability of care. In a pilot data collection of real-time surveillance of suspected suicide, we were notified of 133 deaths by mental health trusts in England between 23 March and 30 September 2020. Most deaths occurred in community settings, and over a third of clinicians reported disruption to the patient’s usual mental health care.
We suggest measures to help suicide prevention during the pandemic are:
- support for those who are anxious, isolated or lonely – a common feature of these deaths;
- a focus on patients who are receiving care under community services, as well as in acute settings;
- minimising disruption to usual care where possible, making use of digital technology where this is appropriate.
Suicide prevention in mental health services
Our findings show there were over 1,600 suicides by people under mental health care in 2018. We recommend healthcare organisations use the Safer Services (PDF) NCISH toolkit to self-assess their services against our ten key elements of safer care for patients.

Find out more
Contact Us
+44 (0) 161 306 6000